- Автоматизация
- Антропология
- Археология
- Архитектура
- Биология
- Ботаника
- Бухгалтерия
- Военная наука
- Генетика
- География
- Геология
- Демография
- Деревообработка
- Журналистика
- Зоология
- Изобретательство
- Информатика
- Искусство
- История
- Кинематография
- Компьютеризация
- Косметика
- Кулинария
- Культура
- Лексикология
- Лингвистика
- Литература
- Логика
- Маркетинг
- Математика
- Материаловедение
- Медицина
- Менеджмент
- Металлургия
- Метрология
- Механика
- Музыка
- Науковедение
- Образование
- Охрана Труда
- Педагогика
- Полиграфия
- Политология
- Право
- Предпринимательство
- Приборостроение
- Программирование
- Производство
- Промышленность
- Психология
- Радиосвязь
- Религия
- Риторика
- Социология
- Спорт
- Стандартизация
- Статистика
- Строительство
- Технологии
- Торговля
- Транспорт
- Фармакология
- Физика
- Физиология
- Философия
- Финансы
- Химия
- Хозяйство
- Черчение
- Экология
- Экономика
- Электроника
- Электротехника
- Энергетика
o Wolff-Parkinson-White syndrome
o Wolff-Parkinson-White syndrome
Long-QT syndrome → torsade de pointes Long-QT syndrome can lead to V-fib directly, or may evolve to torsade de pointes tachycardia, which commonly leads to V-fib, syncope, and/or sudden cardiac death.
o
References: [1]
NOTES
FEEDBACK
Pathophysiology
· Normal electrical conduction can be disrupted by re-entry
→ chaotic, circulating excitation of the myocardium ( = ventricular fibrillation ) → simultaneous contractions at multiple foci → insufficient cardiac output → hemodynamic collapse → loss of consciousness and possibly death (sudden cardiac death)
· Re-entry can be caused by
o Changes to the conduction pathway (e. g., unexcitable scar tissue as a result of past myocardial infarction)
o Abnormal pattern of excitation, for example:
§ If the period of activation and recovery of myocardial cells
becomes greater than the duration of an action potential (as in long-QT syndrome )
§ If excitation occurs outside of the normal pattern of activation ( premature ventricular complex, PVC)
References: [1][2][3]
NOTES
FEEDBACK
Clinical features
· Possible early signs
o Chest pain
o Palpitation
o Fatigue
o Shortness of breath
o Dizziness
· Ultimately: loss of consciousness, death
References: [1][4]
NOTES
FEEDBACK
Diagnostics
ECG findings
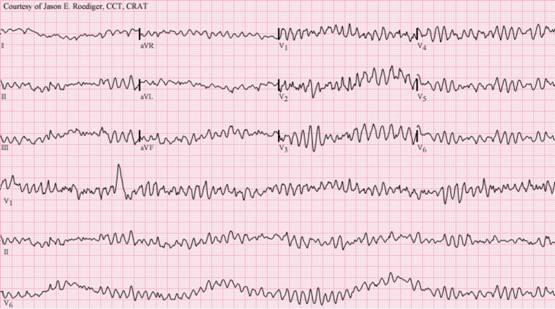
· Ventricular fibrillation
o Commonly preceded by ventricular tachycardia
o General appearance
§ Arrhythmic, fibrillatory baseline, usually > 300 bpm
§ Erratic undulations with indiscernible QRS complexes
§ No atrial P waves
· Ventricular flutter: ventricular rates of ∼ 240–300 bpm
o Frequently transitions to V-fib
· 
|
|
|
© helpiks.su При использовании или копировании материалов прямая ссылка на сайт обязательна.
|